How do Heart Attacks Happen?

In a prior blog entry we discussed stress tests and who should have one so this week I thought it would be useful to go over what a heart attack is and how it occurs.
We've all heard stories of people who have had heart attacks. Maybe a family member had some chest pain and went to his doctor. He had been having chest pains off and on for a while but never told anyone until one day they got too painful to ignore. His doctor admitted him to the hospital and after a series of tests they told him he had a heart attack. A few days later he was released home to his family's care and although he has to make some changes to his lifestyle and take new medications he seems to be back to his old self.
We've all heard stories of people who have had heart attacks. Maybe a family member had some chest pain and went to his doctor. He had been having chest pains off and on for a while but never told anyone until one day they got too painful to ignore. His doctor admitted him to the hospital and after a series of tests they told him he had a heart attack. A few days later he was released home to his family's care and although he has to make some changes to his lifestyle and take new medications he seems to be back to his old self.
Contrast that with your friend. He was only 45 and the picture of health. He had no history of any chest pains at all in the past and you had just gone out running with him the day before. Then out of nowhere it happened. One minute he was trimming his bushes and the next he was clutching his chest. His wife called 911 but as hard as the paramedics tried they couldn't revive him.
These are two extremes of the spectrum. What exactly happens when you have a heart attack and why do some people survive their heart attacks when others do not? Understanding how these things occur is not just an academic exercise. Knowing how a heart attack occurs can help us understand what we can do to prevent them.
These are two extremes of the spectrum. What exactly happens when you have a heart attack and why do some people survive their heart attacks when others do not? Understanding how these things occur is not just an academic exercise. Knowing how a heart attack occurs can help us understand what we can do to prevent them.
Anatomy of a Heart Attack
While heart attacks seem to come on suddenly, they never come out of nowhere. The patient may or may not have had some warning signs but the process that leads to the heart attack started many years before the final event.

Studies done on soldiers killed in the Vietnam war showed that even at ages as young as 18 men had small cholesterol deposits in their arteries known as fatty streaks. This tells us that the process which ultimately leads to the formation of a dangerous cholesterol deposit most likely starts early and develops over many decades.
Deposits start to develop when LDL cholesterol particles (commonly referred to as "bad" cholesterol) migrate below the inner layers of the artery wall. The accumulation of these particles then attracts a type of white blood cell known as a macrophage. Macrophages engulf the LDL particles and then transform into foam cells. Over time the foam cells release their cholesterol which accumulates beneath the surface of the artery forming an atheroma. The atheroma is surrounded by an overgrowth of smooth muscle cells as well as foam cells and other inflammatory cells creating a complex structure we call a plaque.
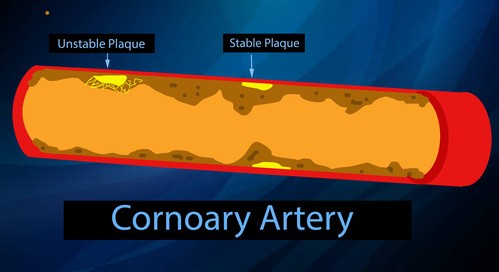
Eventually the plaque may grow in size and the composition of the plaque can change. It may have a solid stable composition or alternatively it can become a very inflamed and unstable structure that might rupture at any time.
Deposits start to develop when LDL cholesterol particles (commonly referred to as "bad" cholesterol) migrate below the inner layers of the artery wall. The accumulation of these particles then attracts a type of white blood cell known as a macrophage. Macrophages engulf the LDL particles and then transform into foam cells. Over time the foam cells release their cholesterol which accumulates beneath the surface of the artery forming an atheroma. The atheroma is surrounded by an overgrowth of smooth muscle cells as well as foam cells and other inflammatory cells creating a complex structure we call a plaque.
Eventually the plaque may grow in size and the composition of the plaque can change. It may have a solid stable composition or alternatively it can become a very inflamed and unstable structure that might rupture at any time.
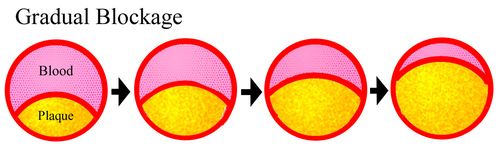
There is more than one way for a heart attack to occur. A person who has a history of chest pains that come on with exertion and then has a heart attack may have had a plaque that has gradually increased in size over years or even decades. As the opening through the artery becomes smaller and smaller the patient may start to notice chest pains when he engages in activities that make increased demands on the heart. The harder the heart works the more oxygenated blood it needs and if the artery becomes too narrow it can't deliver enough blood to meet the hearts needs. This type of pain is called angina. Initially the person may notice this only when he is climbing a steep hill or running but with time it might happen even when he is walking a few blocks on level ground. In severe cases patients may not be able to walk even a few steps to the bathroom without having angina symptoms.
If blood flow to an area of the heart is gradually reduced "collateral" arteries may form. These are additional blood vessels that grow into the area to make up for some of the loss of blood flow as the main artery became clogged. Collateral arteries usually don't provide as much blood flow as the original artery and they don't always form but when they do they are like natures own bypass operation just without the hospital stay or the bill. When the artery finally gets too narrow or closes completely there will be some damage to the heart muscle but it is often less severe than if the artery closes off suddenly and in most cases the patient will have had some warning because he most likely had angina for days, weeks, or years before the event. Approximately 25% of heart attacks occur this way.
If a patient is having chest pains when they exert themselves a doctor may order a stress test. If the stress test is abnormal they will then do an angiogram and if that shows a blockage the doctor may place a stent to open the narrowed area or in some cases bypass surgery may be required.
If blood flow to an area of the heart is gradually reduced "collateral" arteries may form. These are additional blood vessels that grow into the area to make up for some of the loss of blood flow as the main artery became clogged. Collateral arteries usually don't provide as much blood flow as the original artery and they don't always form but when they do they are like natures own bypass operation just without the hospital stay or the bill. When the artery finally gets too narrow or closes completely there will be some damage to the heart muscle but it is often less severe than if the artery closes off suddenly and in most cases the patient will have had some warning because he most likely had angina for days, weeks, or years before the event. Approximately 25% of heart attacks occur this way.
If a patient is having chest pains when they exert themselves a doctor may order a stress test. If the stress test is abnormal they will then do an angiogram and if that shows a blockage the doctor may place a stent to open the narrowed area or in some cases bypass surgery may be required.

Many heart attacks do not happen through a gradual blockage of the artery though. Plaques are very complex structures. As we discussed above, the center is composed of cholesterol but there is a surrounding layer of smooth muscle cells and foam cells forming an overlying cap. In some cases the cap may be a stable structure but in other cases it's more fragile. Inflammation is thought to play an important role in the formation of plaques and the more inflammation there is the more unstable the plaque may be. In these cases the plaque may rupture and when it does the body treats it much the same way it treats a tear in the artery wall. The body's clotting system becomes activated and within minutes a clot forms at the site of the rupture. The clot grows and eventually obstructs the remaining opening in the artery leading to a heart attack. About 75% of heart attacks occur in this way.
In these cases there is often no warning because prior to the rupture there was good blood flow through the artery. In addition, because the blockage happened so suddenly there are usually no collateral arteries. For this reason the damage may be more severe, although the extent of damage also depends on the size of the artery that was blocked.
In these cases there is often no warning because prior to the rupture there was good blood flow through the artery. In addition, because the blockage happened so suddenly there are usually no collateral arteries. For this reason the damage may be more severe, although the extent of damage also depends on the size of the artery that was blocked.
This may explain why patients can sometimes have a normal stress test one day and have a heart attack the next. No stress test can detect whether a plaque is unstable and about to rupture. They can only indirectly determine if the opening around the plaque is allowing enough blood to flow through the artery. A plaque that blocks 30-40% of the artery can go completely undetected but yet if it is unstable and ruptures it may result in a 100% blockage minutes later. CT angiograms ( also known as ultra-fast CT's or 64 slice CT's) and calcium scores all suffer from the same shortcoming. They are unable to detect small unstable plaques that are responsible for many of the sudden heart attacks we hear about.
You've had a heart attack. Why do some people survive relatively unscathed and others do not?
As we saw above, survival after a heart attack may depend on how the heart attack occurs, but there are other factors that can affect the outcome also.
Heart attacks usually involve just a single artery that supplies a portion of the heart. The bigger the artery the more the damage when that artery is obstructed. If too large an area is damaged the heart does not have enough working muscle to pump blood effectively. When that happens even the parts of the heart with good arteries may not get enough blood flow and those areas will be damaged too. Within a matter of seconds or minutes the entire heart will be starved for oxygenated blood and may just stop pumping.
Sometimes even small arteries can cause fatal heart attacks. The heart is more than just a pump made of muscle. It also has an electrical system made up of specialized muscle cells that conduct electrical signals like wires. In order for a healthy heart to pump efficiently the muscle fibers that make up the top chambers need to contract in unison to force blood into the bottom chambers. After a brief delay the muscle fibers in the bottom chambers all have to contract together at the right time to force blood out of the heart to the lungs and the rest of the body. After another delay the whole process starts over. For this to work properly the hearts electrical system has to properly synchronize the entire sequence of events. If a heart attack occurs in a crucial spot it may damage the "wires" that conduct these signals around the heart. The heart will then enter a chaotic rhythm that doesn't allow it to pump blood effectively. Instead of a well coordinated muscular pump the heart may move like a disorganized bag of worms. There are several types of irregular heart beats (also called arrhythmias) that can develop such as Ventricular fibrillation, Ventricular tachycardia, Electrical mechanical dissociation, and eventually asystole. All of these can be fatal if not corrected quickly.
If the irregular rhythm is not corrected in a short period of time the lack of blood flow will lead to further and possibly irreversible damage. When doctors use a defibrillator to "shock" a patient that has gone into cardiac arrest they are attempting to correct one of these by "rebooting" the hearts electrical system in hopes that it will start back up in a normal rhythm.
Heart attacks usually involve just a single artery that supplies a portion of the heart. The bigger the artery the more the damage when that artery is obstructed. If too large an area is damaged the heart does not have enough working muscle to pump blood effectively. When that happens even the parts of the heart with good arteries may not get enough blood flow and those areas will be damaged too. Within a matter of seconds or minutes the entire heart will be starved for oxygenated blood and may just stop pumping.
Sometimes even small arteries can cause fatal heart attacks. The heart is more than just a pump made of muscle. It also has an electrical system made up of specialized muscle cells that conduct electrical signals like wires. In order for a healthy heart to pump efficiently the muscle fibers that make up the top chambers need to contract in unison to force blood into the bottom chambers. After a brief delay the muscle fibers in the bottom chambers all have to contract together at the right time to force blood out of the heart to the lungs and the rest of the body. After another delay the whole process starts over. For this to work properly the hearts electrical system has to properly synchronize the entire sequence of events. If a heart attack occurs in a crucial spot it may damage the "wires" that conduct these signals around the heart. The heart will then enter a chaotic rhythm that doesn't allow it to pump blood effectively. Instead of a well coordinated muscular pump the heart may move like a disorganized bag of worms. There are several types of irregular heart beats (also called arrhythmias) that can develop such as Ventricular fibrillation, Ventricular tachycardia, Electrical mechanical dissociation, and eventually asystole. All of these can be fatal if not corrected quickly.
If the irregular rhythm is not corrected in a short period of time the lack of blood flow will lead to further and possibly irreversible damage. When doctors use a defibrillator to "shock" a patient that has gone into cardiac arrest they are attempting to correct one of these by "rebooting" the hearts electrical system in hopes that it will start back up in a normal rhythm.
Preventing Heart Attacks - Using what we know about how heart attacks occur to make smart choices.
Most people have heard the advice. Keep your cholesterol low, don't smoke, control high blood pressure, keep blood sugar under control and exercise regularly. All of these things do indeed affect your risk for a heart attack. Each one of these risk factors increases inflammation in the arterial wall which then promotes the formation of plaques. The more of these pro-inflammatory risk factors that you have the greater the chance that you will develop a problem. As bad as diabetes is, if you add high blood pressure and smoking to the mix the risk of heart disease will go up dramatically. The same is true for all the risk factors. The more you have the greater your risk.
Its thought that one of the ways that cholesterol medications reduce the risk of heart attacks is through an anti-inflammatory effect. Medications like Lipitor, Zocor, Crestor, and other such "statin" drugs will certainly lower bad cholesterol levels but other unrelated medications which also lower LDL do not reduce the risk of heart disease to the same degree as statins leading some to believe that these drugs may have a secondary anti-inflammatory effect in addition to their cholesterol lower benefits.
Genetics also plays a big role but unfortunately we can't do anything about this risk factor. For good or bad we don't have a choice about the parents we get. Luckily genetics is not as simple as "dad had a heart attack so you're going to have one". You're not a clone of your parents but a unique 50/50 combination of both of their genes. No matter which parent you seem to "take after" you are exactly half mom and half dad. While having a parent with heart disease does increase your risk no one can tell you what effect your unique mixture of genes will have on your health. Its possible you may have inherited some good genes from dad and not the bad ones or perhaps mom has a gene that counters the bad effects of a gene for heart disease that dad gave you. No one knows and no one can tell you. Youre best bet is to fix the things you have control over.
Its thought that one of the ways that cholesterol medications reduce the risk of heart attacks is through an anti-inflammatory effect. Medications like Lipitor, Zocor, Crestor, and other such "statin" drugs will certainly lower bad cholesterol levels but other unrelated medications which also lower LDL do not reduce the risk of heart disease to the same degree as statins leading some to believe that these drugs may have a secondary anti-inflammatory effect in addition to their cholesterol lower benefits.
Genetics also plays a big role but unfortunately we can't do anything about this risk factor. For good or bad we don't have a choice about the parents we get. Luckily genetics is not as simple as "dad had a heart attack so you're going to have one". You're not a clone of your parents but a unique 50/50 combination of both of their genes. No matter which parent you seem to "take after" you are exactly half mom and half dad. While having a parent with heart disease does increase your risk no one can tell you what effect your unique mixture of genes will have on your health. Its possible you may have inherited some good genes from dad and not the bad ones or perhaps mom has a gene that counters the bad effects of a gene for heart disease that dad gave you. No one knows and no one can tell you. Youre best bet is to fix the things you have control over.
I have often heard people comment that " My uncle smoked his whole life and lived to be 100" or "My friend ran marathons and ate healthy and still had a heart attack when he was 45". This is possible. No one knows for sure what their genetic makeup will lead to. Some of us are blessed and others are not but we have no way of knowing which camp we fall in to.
We have to keep in mind that there are no guarantees in life. Yes you could eat a Big Mac every day, smoke like a chimney and live to be 100. You could also hold onto a metal flag pole in a thunder storm and not get hit by lightening but how many times would you like to try that? Would you prefer to play a slot machine that gives you a 1 in 10 chance of winning or one that gives you a 4 in 10 chance? Staying healthy is not about guarantees, its about stacking the odds in your favor. We can't control our genes but virtually everything else IS under our control.
There are pages on this website that address most of the cardiac risk factors including diabetes, cholesterol, hypertension, and smoking. If you want help with any of these problems take a look at the information on these links.
One last thing, patients often ask if they should have a stress test to prevent a possible heart attack. Someone who is having chest pains should certainly seek the advice of their doctor but if there are no symptoms then think about what we discussed above and read last weeks blog for a full explanation of why a stress test might not be a good idea. There is also another page on this web site that addresses many of the other "heart" tests you may have heard about. You can access that at this link: Screening for Heart Disease
As always if you have further questions please consult your physician.
We have to keep in mind that there are no guarantees in life. Yes you could eat a Big Mac every day, smoke like a chimney and live to be 100. You could also hold onto a metal flag pole in a thunder storm and not get hit by lightening but how many times would you like to try that? Would you prefer to play a slot machine that gives you a 1 in 10 chance of winning or one that gives you a 4 in 10 chance? Staying healthy is not about guarantees, its about stacking the odds in your favor. We can't control our genes but virtually everything else IS under our control.
There are pages on this website that address most of the cardiac risk factors including diabetes, cholesterol, hypertension, and smoking. If you want help with any of these problems take a look at the information on these links.
One last thing, patients often ask if they should have a stress test to prevent a possible heart attack. Someone who is having chest pains should certainly seek the advice of their doctor but if there are no symptoms then think about what we discussed above and read last weeks blog for a full explanation of why a stress test might not be a good idea. There is also another page on this web site that addresses many of the other "heart" tests you may have heard about. You can access that at this link: Screening for Heart Disease
As always if you have further questions please consult your physician.
Recent
Should You Get a Multi-Cancer Early Detection Blood Test?
May 22nd, 2026
Shredded Is Not the Same as Healthy
May 13th, 2026
Measels: Who needs to update their vaccine?
May 12th, 2026
Lung Cancer - Who should get screened (Update)
May 12th, 2026
Are You Really Allergic to Penicillin? The Truth Might Surprise You
January 19th, 2025
Archive
2026
2024
May
Ozempic - Obesity cure or panacea?GMO's (Genetically Modified Organisms) - Are they truly "Frankenfoods" or our best hope for feeding a hungry world?The Drip Dilemma: Why Healthy People Should Steer Clear of IV TherapyLung Cancer Screening - Is it time to get a CT scan?The Whole Truth Behind Whole Body MRI Scans – Overhyped, Overpriced, and Overrated!Understanding Sinus Infections: Beyond the Common ColdAbdominal Aortic Aneurysms: What You Need to Know
June
2014
March
May
2013
July
August
October
November
Omega 3's (Fish Oil and Flax Seed Oil) who should take them?How do you save a life ? - Just swab your cheekNew Cholesterol Guidelines - What's changed and what does it mean for you?Antibiotics and Probiotics- Why you shouldn't take either without a good reasonPreventing Heart Disease with almonds- Is this study Nuts?