Welcome
Hello and Welcome. This article was written to help our patients understand the COVID 19 vaccines that are now available. There is an enormous amount of misinformation about both COVID 19 and the new vaccines on the internet and from other sources as well. My goal here is to replace fear with facts so that you can make an educated decision about the vaccine. This is just a summary of the important facts you should know and can't possibly cover everything but we hope it will provide you with the basic information to guide you and help you formulate any additional questions. After viewing this information please discuss any remaining questions with your physician so you can make the choice that is best for you.
How does SARS CoV2 infect our cells
To understand how these vaccines work lets first look at how the Coronavirus that causes COVID 19 attacks the body and enters the cells
The Coronavirus is an RNA virus. That means it's genetic information is stored as RNA instead of the DNA that our cells use to pass down our genetic information from one generation to the next. The virus starts its attack by binding to one of our cells and fusing with it. Once it has done this it injects its RNA into the cell. Our own cells also use a type of RNA called messenger RNA or mRNA to copy instructions from the DNA and then carry them to our ribosomes where those instructions are used to make essential proteins.
The Coronavirus is an RNA virus. That means it's genetic information is stored as RNA instead of the DNA that our cells use to pass down our genetic information from one generation to the next. The virus starts its attack by binding to one of our cells and fusing with it. Once it has done this it injects its RNA into the cell. Our own cells also use a type of RNA called messenger RNA or mRNA to copy instructions from the DNA and then carry them to our ribosomes where those instructions are used to make essential proteins.

Once it has injected its RNA into our cells the virus hijacks our cells ribosomes to make the proteins that it needs to make more virus. Ribosomes are like little protein factories. They use the instructions on the mRNA to build protein molecules from amino acids. The ribosome doesn't know the difference between our mRNA and the viral RNA so it uses the instructions it is given on the viral RNA and produces viral proteins. Some of those proteins are enzymes that go on to make millions of more copies of the viral RNA and also to produce more proteins that are required to build new viruses. These proteins and additional copies of RNA are then assembled into new viruses that leave the cell to go off and infect other cells and the whole process starts all over again.
As soon as the virus invades our cells the body starts mounting its defenses. The one defense that most people have heard about are antibodies but in truth the immune system is far more complex than that and there are many other portions of the immune system that our body uses to defend itself both before and after the antibodies become involved. We won't get into that here for the sake of time but antibodies are a portion of that defense system that vaccines make use of and that's what I want to focus on.

Antibodies are like a lock to a key. Every bacteria and virus has proteins on its surface that are unique to them. In the case of the COVID19 virus, the spike protein is just such a protein. When the body's immune system detects a protein that does not belong there it creates an antibody that will lock onto it. The first time we see a new protein it takes a while for the body to learn how to make that antibody but once it learns how it keeps some of those antibodies around for a while. It also keeps around some T and B cells that remember how to make antibodies and respond should the virus return. That way the next time we are exposed to that virus or bacteria the antibodies can be produced in large numbers much more quickly. It's like building a house. If you need to build another one it will go up much faster the next time if the carpenters who built the first one are still around to help and they have the original blueprints.

How do vaccines work
The idea behind vaccines is that we are giving our body the blueprints to the virus or bacteria so that if we are ever exposed to the actual infection our immune system will know how to make those antibodies immediately which will either prevent the illness altogether or at least end the infection before it causes any damage.
There are many ways to make a vaccine. The first vaccines were weakened versions of live viruses that would cause a mild infection but trigger the same immune response as if we had gotten the real infection. These vaccines were effective but in a very small percentage of patients some of these vaccines can cause the actual illness. Other vaccines are made using a killed version of the virus which has been disrupted and destroyed so it is unable to reproduce but still contains the necessary proteins to produce the immune response. The development of these types of vaccines can take years
mRNA Vaccines
More recently other techniques have been developed to make the development process more efficient. The one that has been most in the news lately has been the mRNA vaccines.
These vaccines work by introducing a small portion of the viral RNA into the body to coax our cells into making a protein. Think of mRNA like a recipe or blueprint. Within our cells are those little factories called ribosomes that were mentioned above. They read the recipe from the strip of mRNA and use it to build a protein that it codes for. In the case of the COVID19 vaccines it codes for a portion of the spike protein. The mRNA is enclosed in a microscopic fat bubble during manufacturing to protect them and to allow them to merge with our cells and get the mRNA inside the cell where it can be used by the ribosomes. When the actual Coronavirus inserts its RNA into the cell that RNA has instructions for many different proteins, but the mRNA in the vaccines is providing instructions only for a portion of the spike protein from the surface of the virus. The vaccine mRNA does not contain any of the code for the other proteins that allow the Coronavirus to make more copies of itself and cause illness.
Once the mRNA is inside the cell the ribosomes use that mRNA to produce the spike proteins and display them on the surface of the cell. Once they are on the surface of the cell the spike proteins are visible to our immune cells which will then start the process of creating and producing antibodies.
These vaccines work by introducing a small portion of the viral RNA into the body to coax our cells into making a protein. Think of mRNA like a recipe or blueprint. Within our cells are those little factories called ribosomes that were mentioned above. They read the recipe from the strip of mRNA and use it to build a protein that it codes for. In the case of the COVID19 vaccines it codes for a portion of the spike protein. The mRNA is enclosed in a microscopic fat bubble during manufacturing to protect them and to allow them to merge with our cells and get the mRNA inside the cell where it can be used by the ribosomes. When the actual Coronavirus inserts its RNA into the cell that RNA has instructions for many different proteins, but the mRNA in the vaccines is providing instructions only for a portion of the spike protein from the surface of the virus. The vaccine mRNA does not contain any of the code for the other proteins that allow the Coronavirus to make more copies of itself and cause illness.
Once the mRNA is inside the cell the ribosomes use that mRNA to produce the spike proteins and display them on the surface of the cell. Once they are on the surface of the cell the spike proteins are visible to our immune cells which will then start the process of creating and producing antibodies.

mRNA is a very fragile molecule that decays within a few hours which is why it has to be packaged in tiny fat bubbles and also why these vaccines have to be kept frozen at very low temperatures. Once inside our body all of the vaccine mRNA is broken down by our enzymes within hours but not before our cells use it to make the proteins required to generate an immune response.

The first two vaccines that were approved were the mRNA vaccines produced by Pfizer and Moderna. They are very similar in most ways. They are both very effective and current studies involving over 30,000 participants in each trial have shown no serious side effects after almost 6 months. Despite this some people are reluctant to take the vaccine. This seems to be due in no small measure to the rapid speed of development but is also due in part to the unfortunate politicization of these vaccines. The rest of this article will be devoted to explaining how scientists were able to develop these vaccines so quickly. There were several factors that I will review here which allowed the process to proceed at a rapid pace while still following the procedures that are always followed to ensure safety.
Other Vaccines
mRNA vaccines are the first to make it to market but there are other technologies being used to create additional vaccines.
- Viral Vector Vaccines - Two vaccines, The Johnson and Johnson vaccine and the Astra Zeneca vaccine use something called a viral vector which uses a harmless adenovirus ( a cold virus ) that has been stripped of its ability to reproduce. These viruses have had their DNA altered so that the code for the spike protein has been added. When they enter the cell that DNA is then transcribed into messenger RNA (mRNA) which is then translated by the cell into the spike protein just the same like what happens with the mRNA vaccines.. The Johnson and Johnson vaccine has been approved for use in the U.S. but the Astra Zeneca vaccine has not yet been approved in U.S. as of this date. CLICK HERE to learn how viral vector vaccines work
- Protein Subunit Vaccines - Several companies are working on vaccines that inject just the spike protein or a portion of it to produce an immune response. Novavax is available in the U.S.
- Live Weakened Virus Vaccines - China and Russia have produced a vaccine made from a weakened version of the COVID19 virus. These are not being used in the U.S. or Europe but have been licensed in other countries. CLICK HERE to learn how attenuated (weakened) virus vaccines are made.
So how did they make this vaccine so quickly?
mRNA technology and the scientists behind it
One of the things that takes a long time with traditional vaccine technology is identifying and developing the virus or portion of a virus to make the vaccine itself. With live virus vaccines It takes a lot of trial and error to weaken a virus so it doesn't cause illness, but not weaken it so much that it fails to stimulate the immune response. Killed virus vaccines also take time to develop because they usually don't trigger as strong an immune response and it can take a long time to identify the correct preparation required to get the desired response. The difference with mRNA technology is that it only requires that the viral genetic code be sequenced which can now be done in days or weeks with current technology. Once that is done the section of the RNA that codes for the surface protein can be synthesized easily and produced in large quantities.
Vaccine companies were willing to take financial risks
Vaccine development is expensive and time consuming. The first trial involves hundreds of people, the next involves thousands, and the final or Phase 3 trial involves tens of thousands of participants. Each phase costs millions or hundreds of millions of dollars. It takes time to design and set up these trials and in between it takes time for the FDA to review and approve each one. Companies generally wait until the first trial has been reviewed before they start the next. This sequential approach adds time to the process but protects the company from making a big investment in the next step if the prior step fails. In the case of COVID19 vaccine companies overlapped the trials to speed the process up although this exposed them to significant financial risk if the vaccine failed.
The government also prioritized the review process.
The same review was used for the COVID vaccines that are required of all vaccines but due to the critical nature of the pandemic the vaccines jumped to the head of the line. They didn't have to wait in line behind other pharmaceuticals like they would in normal times. This eliminated some of the usual delay.
Altruism and Public Engagement
It usually takes a long time to enroll tens of thousands of participants in phase three trials, sometimes years. COVID vaccine trials filled up quickly because people wanted to help and were willing to take a risk if it would save lives.
The Presence of Lots of Disease
When trials are done the participants need to be exposed to the virus in order to know whether the vaccinated group had fewer infections than the placebo group. Its not ethical to intentionally infect people with a deadly virus so instead you send everyone home to live their lives. If there is very little infection in the community it can take a long time for enough participants to get infected in order to see if there is a difference between the vaccinated and placebo groups. With COVID19 unfortunately we had no shortage of infections in the community so vaccine trials were able to get the numbers they needed pretty quickly.
Government Guarantees and Commitments
Governments around the world made a commitment to buy the vaccines before they were even proven to work. This allowed companies to start tooling up manufacturing facilities earlier in the process so that doses were available as soon as the vaccines were approved.
"But I heard...."
Rumors and Misinformation
The internet is an amazing tool but it's also a great source for spreading misinformation. Over that past year I have heard plenty of claims about this vaccine that aren't even remotely true but which have been making the rounds on the internet and social media platforms. Aside from the "It was created too quickly, it couldn't be safe" concern which was addressed above there are several other concerns I've heard patients voice which are based on incorrect information, such as...
The Pfizer COVID-19 vaccine contains the following ingredients:
The Moderna COVID-19 Vaccine contains the following ingredients:
.....As you can see not a single nanotransducer, tracker, animal cell, or fetal cell
Several systems are used in the United States to monitor vaccine safety and detect possible adverse events after vaccination. These systems work together to identify rare side effects, investigate safety signals, and monitor vaccine safety over time.
What side effects are known to occur with COVID-19 vaccines?
While there are a lot of silly claims about these and other vaccines there are some actual side effects everyone should be aware of.
Rare side effects:
NOTE: It's important to note that these rare side effects have not been definitively associated with the vaccines. All of these conditions occur naturally at low rates even in non-vaccinated individuals and all of them occur at much higher rates in patients who are actually infected with COVID19.
- "mRNA vaccines change your DNA" - No, definitely not. Your cells make plenty of their own mRNA and every virus you have ever been infected with has inserted mRNA into your cells. If mRNA could alter our DNA it would be doing it every second of every day in every one of us. Clearly that's not happening. mRNA does not have the ability to change DNA.. It's also important to realize that mRNA does not last very long in the body. Enzymes called ribonucleases rapidly degrade mRNA..
- "There are animal cells in the vaccine" - This is false. No cells of any sort are present in these vaccines and none are used to manufacture them.
- "There are fetal cells in the vaccine" - Again, no. No fetal cells or cells of any kind are used to make mRNA vaccines. Fetal cell cultures that were created in the 1960's were used to develop the J&J vaccines but there are no fetal cells in the actual vaccines.
- "The vaccine can cause infertility" - This is another claim that has not even the slightest basis in fact. There is no evidence from any of the trials of an association between the vaccines and infertility. This rumor was started by a scientist who noticed that the spike protein has 4 amino acids that are similar to a protein which is required for placental attachment to the uterus. But thats just 4 amino acids out of more than 240. Then without any evidence and without a proper understanding of the biology he jumped to the completely unfounded conclusion that an antibody to one would also bind to the other. There is no evidence to support this idea even after more than 180 million have been vaccinated in the U.S. including millions of young women. Keep in mind that if one is infected with COVID19 they will also form antibodies to this same protein so if this were true COVID19 infections would also lead to infertility. Again this is a foolish theory made up by someone without any evidence and which has been disproven by thousands of vaccinated young women who have gotten pregnant.
- "COVID-19 vaccines were developed to control the population through microchip tracking or "nanotransducers" in the human brain". - This is one of the wackiest claims. Nothing even remotely close to this kind of technology exists. There is also no evidence that Bill Gates ever made any comments or statements about any such technology. This is just plain nuts..
- "COVID19 vaccines cause Bell's Palsy" - This has been circulating on social media without proper context. Four people in the Pfizer trial and three in the Moderna trial developed Bell's Palsy. One person in the placebo group also developed Bell's palsy. Bell's palsy is a common condition that results in weakness or paralysis of one side of the face. It usually resolves on its own in a few weeks but the incidence of Bell's palsy in the studies was actually less than the usual background rate of Bell's palsy in the general population which is about 25-35 cases per 100,000 people. So even if the vaccine did absolutely nothing to cause Bell's palsy you would expect that in a group of 30,000 vaccinated people you would have 9 cases of Bell's palsy. Although the FDA will continue to follow and collect data on this issue, claims that the vaccine causes Bell's palsy are not supported by the data we have.
- "People have died from the vaccine" - Again no evidence for this. There were six deaths during the trials but remember this was not just a trial of health 20 yr olds. The goal was to see how the vaccine worked across a large segment of age groups, nationalities and race. Of the 44,000 people in the trial there were six deaths but of those six, four were in the placebo group that got nothing but a tiny salt water injection.. Of the two that died in the vaccine group, one died of heart disease three days after getting the vaccine and the other died of a cardiac arrest 62 days after vaccination. That means there were two deaths out of 22,000 vaccinated individuals but the normal death rate in the U.S. is 723/100,000 people. So the death rate in this trial was far below the normal background death rate. There is no evidence that the vaccine caused any deaths.
- VAERS reports of side effects and deaths - VAERS is the Vaccine Adverse Events Reporting System. This system was setup by the CDC and FDA to detect any evidence of adverse vaccine events after a vaccine goes to market. The system allows anyone to file a report about anyone else. As such VAERS is not verified data and it is not a list of events that were caused by a vaccine. Its is simply a list of reports that someone ( doctor, nurse, patients, patients family or neighbors) submitted about anything that occurred during sometime after they got a vaccine. The information is not useless but it requires the expertise of doctors, scientists, and statisticians to determine if a report is accurate and the events reported raise a significant concern about a vaccine. For example if someone got vaccinated and 2 months later had a car accident (yes there are entries like this) its unlikely that the vaccine caused the event but what about other reports. What if someone has a heart attack a week or two after being vaccinated. For cases where a link seems at least possible, if there are reports of heart attacks after a vaccine we need to look at the unvaccinated population to see what the background rate of heart attacks is. If the rate is the same in the unvaccinated group then the vaccine is not likely to be the cause of the heart attacks. Some antivaccine website boldly claim that tens of thousands of deaths have been caused by COVID vaccines. Reports of 20 or 30 thousand deaths among patients after the covid vaccine therefor need to be looked at in this light. Over 200 million Americans have been vaccinated. These vaccines are not going to prevent all the other things that people normally die from (heart disease, cancer, accidents etc) so we would still expect some of the people in that group to die at some time after the vaccine even if the vaccine is 100% safe. In fact among 200 million people the normal death rate is about 3961 per day in the U.S. If we only care about the number of deaths in the two weeks after vaccination, there would be over 55,000 deaths every two weeks in the U.S. As you can see a report that 30,000 people (out of 200 million) have died within 2 weeks of vaccination may not be very meaningful. and is unlikely related to the vaccine. Despite being fully aware of this, some anitvaccine websites have persisted in misrepresenting VAERS information causing fear and leading to increased rates of vaccine hesitancy and unnecessary deaths from COVID19.
- "I heard you can't take the vaccine if you have allergies" - This is not true and is perhaps a misunderstanding of a statement that people with a history of severe anaphylactic reactions should delay taking the vaccine.. In general, people with a history of environmental allergies, hay fever, or drug or vaccines allergies that result in mild symptoms are not at any greater risk of taking the COVID29 vaccine. Anaphylactic reactions to the COVID19 vaccines are very rare, on the order of about 2-5 people per million.
- "Taking pain killers (Advil, Motrin, Tylenol etc) will reduce the effectiveness of the vaccine" - Studies on some other vaccines in the past showed a mild reduction in antibody production in children if pain killers/fever reducers were taken to reduce symptoms after vaccination but these same studies seemed to show that there was no reduction in the vaccines ability to prevent infection. There is no specific data on the affect of any of these drugs on the response to the COVID19 vaccines. While premedication is generally not necessary or wise there is no significant data to suggest against the use of these medications if needed to treat body aches, headaches, or fever.
- "Healthcare workers are reluctant to get the vaccine" - This is a distortion of the actual facts and implies that doctors are not confident in the vaccine. That is completely false. While there are hospital workers who have been hesitant to get the vaccine that hesitancy is mostly among non-professionals. Almost all physicians have gotten the vaccine and the more educated a physician is about these vaccines the more likely they are to be vaccinated. Nurses have a lower level of vaccine knowledge on the whole and they are slightly less likely to be vaccinated. The great majority of "healthcare workers" who have declined the vaccine are people without any medical training at all. These healthcare workers work as Nurses Aids, Cleaning Personnel, Transporters etc. The more people know about this vaccine the more likely they are to get vaccinated.
- I didn't think COVID "was a thing anymore". Isn't it just like a cold? - COVID is definitely still a thing and its not like a cold. Its more like the flu now. in 2024 there were still about 47,000 deaths in the US from COVID which is in the same range as the annual deaths we see from the flu. Much like the flu and different from a cold it also results in a large number of lost work days because the illness can be very disabling with fever, body aches, cough and sore throat. It's also highly contagious (twice as contagious as the flu) and it mutates regularly like the flu requiring at least an annual vaccine update to reduce susceptibility.
- "We don't know what's in these vaccines" - We know exactly what is in all of these vaccines. Here is the list.......
The Pfizer COVID-19 vaccine contains the following ingredients:
- mRNA
- Four lipids: Three types of fat molecules that provide a protective bubble around the mRNA, and cholesterol.
- Sucrose (sugar)
- Four salts: potassium chloride, monobasic potassium phosphate, basic sodium phosphate dihydrate and sodium chloride (table salt).
- mRNA
- Lipids (SM-102, polyethylene glycol [PEG] 2000 dimyristoyl glycerol [DMG], cholesterol, and 1,2-distearoyl-sn-glycero-3-phosphocholine [DSPC])
- Sucrose (sugar)
- Stabilizers: The remaining ingredients, including acids (acetic acid), acid
stabilizers (tromethamine and tromethamine hydrochloride),
salt (sodium acetate), and sugar (sucrose) all work together to
maintain the stability of the vaccine after it’s produced.
.....As you can see not a single nanotransducer, tracker, animal cell, or fetal cell
- "I heard that 1 million people died from the covid vaccine" - That is a complete falsification. There is no evidence to support that claim at all. A major jump in the narrative happened in 2021 when claims circulated that 45,000 Americans had died from the vaccine. That number came from an affidavit submitted in a lawsuit connected to a group called America's Frontline Doctors. This is a small group of doctors who have made a number of unsubstantiated claims and promoted disproven treatments for covid. The estimate was attributed to an unnamed “whistleblower” and attorney Thomas Renz. Fact-checkers later found there was no verifiable evidence supporting the number.
From there, the numbers escalated online:- “45,000 deaths”
- then “hundreds of thousands”
- then “millions”
- and eventually claims of “17 million deaths worldwide.”
Several systems are used in the United States to monitor vaccine safety and detect possible adverse events after vaccination. These systems work together to identify rare side effects, investigate safety signals, and monitor vaccine safety over time.
- Vaccine Adverse Event Reporting System (VAERS)
A national early-warning system co-managed by the Centers for Disease Control and Prevention and the U.S. Food and Drug Administration. Healthcare professionals, patients, and manufacturers can submit reports of health problems occurring after vaccination. VAERS is useful for detecting potential safety signals but cannot by itself prove that a vaccine caused an event. - Vaccine Safety Datalink (VSD)
A collaboration between the CDC and several large healthcare organizations. It uses electronic health records from millions of patients to compare vaccinated and unvaccinated populations and study whether certain adverse events occur more often after vaccination. - Clinical Immunization Safety Assessment Project (CISA)
A network of vaccine safety experts and academic medical centers that performs detailed clinical evaluations of complex or rare vaccine adverse events and provides expert consultation to clinicians. - Biologics Effectiveness and Safety System (BEST)
An FDA system that analyzes large healthcare databases, including insurance claims and electronic medical records, to rapidly evaluate possible vaccine safety concerns in near real time. - v-safe
A smartphone-based system developed by the CDC that sends surveys to vaccine recipients after vaccination to monitor symptoms and health impacts. It was widely used during the COVID-19 vaccination campaign. - Post-licensure manufacturer surveillance
Vaccine manufacturers are required to continue monitoring safety after approval and report adverse events to regulatory agencies. They may also conduct post-marketing safety studies. - International monitoring systems
Organizations such as the World Health Organization coordinate global vaccine safety monitoring and collect reports from multiple countries to identify rare adverse events that may not be apparent within a single nation.
What side effects are known to occur with COVID-19 vaccines?
While there are a lot of silly claims about these and other vaccines there are some actual side effects everyone should be aware of.
- Headache, fatigue, chills, low grade fever, or body aches - A significant percentage of the patients in the trials developed some of these symptoms. These are common with lots of vaccines because any time we activate the immune response these are the symptoms that tell us the immune system is working. The good news is the symptoms usually last only a day and respond well to medications like Ibuprofen (Advil or Motrin) or Acetaminophen (Tylenol).
- Allergic reaction - There have been a handful of patients who have had allergic reactions to the vaccines so far. The overall risk is extremely low (about 2-5 people per million) and most of these patients had a history of severe allergic reactions in the past. Their reaction was quickly reversed with an Epipen. It's not yet clear if the allergic reaction was triggered by the vaccine or the latex stopper in the vial but as a precaution patients with a history of anaphylaxis in the past are advised not to take the vaccine until we know more.
Rare side effects:
- Blood clots - These have occurred only in women who have taken the Johnson and Johnson vaccine or the Astra Zeneca Vaccine and occur in extremely rare cases (1 in 500,000). Blood clots are about 100 times more common from a COVID infection than from the vaccine
- Myocarditis and Pericarditis - These conditions are an inflammation of the heart muscle or the sack around the heart respectively. Rare cases of this have been seen in some patients who have gotten the mRNA vaccines. The condition is usually mild and most patients recover completely. The incidence of Myocarditis were 40.6 cases per million second doses of mRNA COVID-19 vaccines administered to males aged 12−29 years. The incidence of Myocarditis and Pericarditis are about 6 times more common from COVID infections than from the vaccines
- Guillain Barre - This is a neurologic disorder that results in gradual weakening of the voluntary muscles. Mild cases only cause isolated mild weakness but more severe cases can paralyze the respiratory muscles and require ventilator support.. This condition has been seen only in association with the J&J vaccine and occurred in about 1 in 125,000 patients.
NOTE: It's important to note that these rare side effects have not been definitively associated with the vaccines. All of these conditions occur naturally at low rates even in non-vaccinated individuals and all of them occur at much higher rates in patients who are actually infected with COVID19.
Special Considerations
Pregnant Women and Breastfeeding Women
- From ACOG ( the American College of Obstetrics and Gynecology) -
- "ACOG recommends COVID-19 vaccines be offered to lactating individuals similar to non-lactating individuals when they meet criteria for receipt of the vaccine based on prioritization groups outlined by the ACIP. While lactating individuals were not included in most clinical trials, COVID-19 vaccines should not be withheld from lactating individuals who otherwise meet criteria for vaccination. Theoretical concerns regarding the safety of vaccinating lactating individuals do not outweigh the potential benefits of receiving the vaccine. There is no need to avoid initiation or discontinue breastfeeding in patients who receive a COVID-19 vaccine. "
- ACOG recommends that COVID-19 vaccines should not be withheld from pregnant individuals who meet criteria for vaccination based on ACIP-recommended priority groups. While safety data on the use of COVID-19 vaccines in pregnancy are not currently available, there are also no data to indicate that the vaccines should be contraindicated, and no safety signals generated from DART studies for the Pfizer-BioNtech vaccine. Therefore, in the interest of allowing pregnant individuals who would otherwise be considered a priority population for a vaccine approved for use under EUA, make their own decisions regarding their health, ACOG recommends that pregnant individuals should be free to make their own decision in conjunction with their clinical care team..
- From AAP (the American Academy of Pediatrics) - No pregnancy related data have yet been released. Typically, in large trials, there are some inadvertent pregnancies. They will be followed for birth outcomes. Pregnancy and breastfeeding will probably not be contraindications to receiving COVID-19 vaccine; however, there is no safety data in the pregnant woman, her fetus or infants at this time. While these vaccines were not specifically tested in breastfeeding women, it is not likely (based on the mechanisms of action of the vaccines in US trials) that there would be any risk to the child.
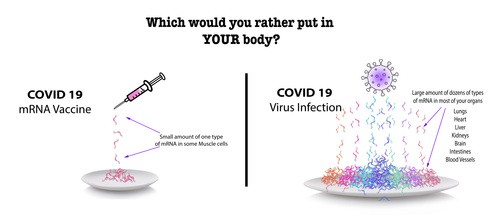
Conclusion
All of these processes are the kind of things that allowed the vaccines to be produced more quickly but none of these things cut corners or compromised safety. These vaccines have been studied in more people, with more involvement by more government agencies around the world and with more transparency than any vaccine in history. By the time the general public was offered the vaccine more than twenty million additional health care workers and nursing home patients had received the vaccine and more than a year had passed since the first vaccines were given to trial participants. The public has never received a vaccine that was more studied than this one has been and will continue to be. The diagram below summarizes in a single picture what this decision really come down to..
How to get Vaccinated
If you live in NY, the State the sites below can be used to schedule an appointment for a free COVID19 vaccine. Some hospital systems including NYU and Northwell allow their patients to schedule a vaccine through their app.
- Enter your zip code and choose the vaccine you want - https://www.vaccines.gov/search/
- Text your zip code to GETVAX ( or to 438829) to get a list of vaccine locations in your area
- CVS: https://www.cvs.com/immunizations/covid-19-vaccine?icid=coronavirus-lp-nav-vaccine
- Walgreens: https://www.walgreens.com/topic/promotion/covid-vaccine.jsp?ext=gooFY21_COVID+Vaccine_NB_BMMCOVID_NB_COVID+Vaccine_BMM_%2Bcovid%20%2Bvaccine&gclsrc=aw.ds&&gclid=CjwKCAiAjp6BBhAIEiwAkO9WumKczd6E2fptEwON3Q5pABCW_MYV-UJFDB9ovN_XFUB6Ycs5unJqbxoC-LwQAvD_BwE